

table of contents
This guide is written for civilian readers, Stop the Bleed participants, law enforcement personnel, and anyone building a trauma kit — no prior military or medical background assumed. Operational personnel should cross-reference with their unit’s current protocols.
What Is TCCC?
In October 1993, during the Battle of Mogadishu, U.S. forces suffered 18 killed and 73 wounded in one of the most intense urban combat engagements since Vietnam. The after-action medical review identified a troubling pattern: a significant number of the deaths were potentially preventable. The injuries were survivable. What was missing was a systematic framework for applying the right intervention in the right sequence under fire.
That analysis, led by Dr. Frank Butler and Dr. John Hagmann and published in 1996 in Military Medicine, became the foundation of Tactical Combat Casualty Care—TCCC. The core insight was straightforward: the leading cause of preventable death on the battlefield was not inadequate evacuation or hospital care. It was uncontrolled compressible hemorrhage in the first minutes after injury, before any medic arrived. Stopping that bleeding—fast, by whoever was nearby—was what saved lives.
TCCC is a standardized, evidence-based framework for pre-hospital trauma care in tactical environments. It defines what to do, in what order, when to do it, and — just as importantly — what not to do when time and resources are limited and the threat is still active.
Since 1996, TCCC has been formally adopted by the U.S. military and has been credited, alongside improved body armor and rapid evacuation, with reducing the battlefield case fatality rate to historically low levels. It is now the standard of care for U.S. Army, Navy, Air Force, and Marine Corps medical training, and its principles have been adapted for law enforcement (TECC — Tactical Emergency Casualty Care) and civilian hemorrhage control (Stop the Bleed).
What does TCCC stand for? Tactical Combat Casualty Care. It is maintained and updated by the Committee on Tactical Combat Casualty Care (CoTCCC), which publishes revised guidelines periodically as new evidence emerges from combat experience and clinical research. The most recent update was January 2024.
The Three Phases of TCCC
TCCC organizes trauma care into three distinct phases based on the tactical situation—specifically, the level of ongoing threat and what resources are available. The phase determines what treatment is appropriate. Doing too much in Phase 1 can get the rescuer killed. Doing too little in Phase 2 wastes a window that may not come back.
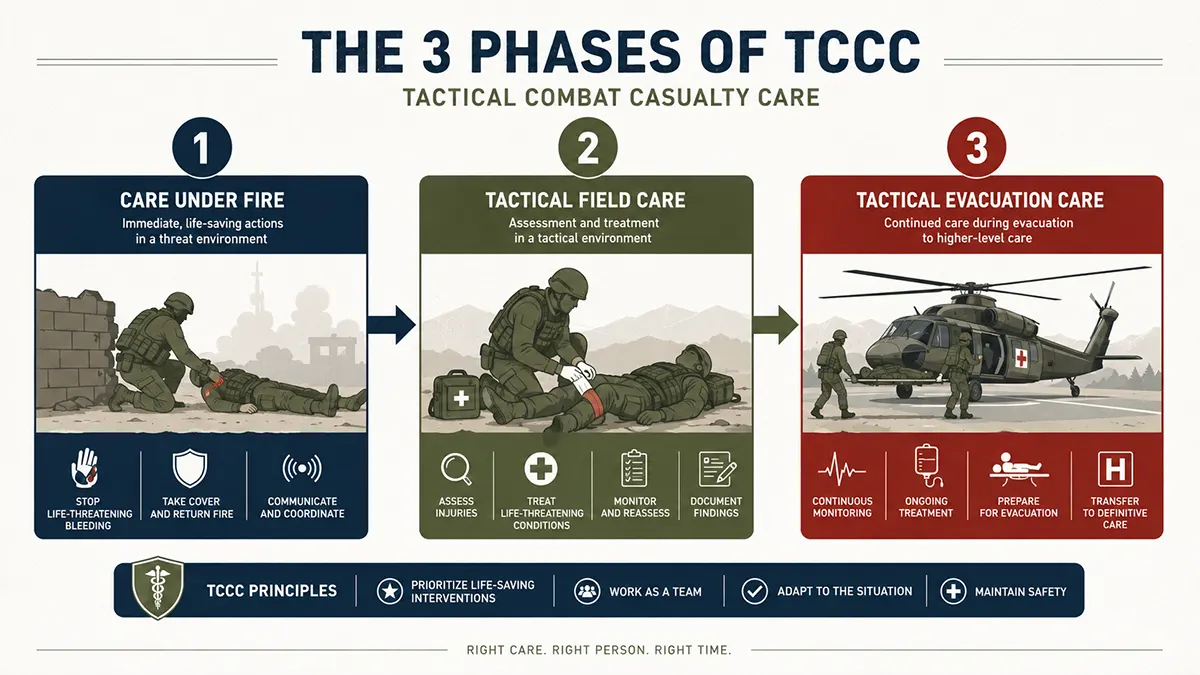
Phase 1 — Care Under Fire
Care Under Fire covers the period when both the casualty and the rescuer are exposed to direct hostile fire. The threat is active, the position is not secure, and every second spent treating rather than moving or returning fire increases the danger to everyone present.
In this phase, the treatment options are deliberately narrow:
- Return fire and take cover—mission and force protection come first; a rescuer who becomes a second casualty helps no one
- Direct the casualty to self-aid if conscious—shout instructions; a conscious person can apply their own tourniquet faster than you can reach them under fire
- Apply a tourniquet for life-threatening limb hemorrhage—this is the one intervention TCCC mandates in Phase 1; it takes under 60 seconds and can be applied over clothing
- Move the casualty to cover—only when tactically feasible; never move into a zeroed-in position
Everything else waits. Airway management, wound assessment, IV access — none of it happens in Phase 1. The calculus is simple: a tourniquet applied in 30 seconds under fire is worth more than a comprehensive assessment completed after the rescuer is hit.
Phase 1 equipment minimum: One tourniquet on every person entering a tactical environment, staged on the body for one-handed self-application. Not in a bag. Not in a vehicle. On the body.
Phase 2 — Tactical Field Care
Tactical field care begins when the immediate threat has been suppressed or the casualty has been moved to a position of relative cover. The situation may not be fully secure — re-engagement is possible — but there is enough time to conduct a systematic assessment and treat life-threatening injuries in priority order.
This is where the MARCH algorithm is applied. MARCH is the core decision sequence of TCCC—a structured, repeatable scan that addresses threats to life in the order they will kill fastest. It is covered in detail in the next section.
Additional priorities in Tactical Field Care include disarming any casualty with altered mental status before treatment—a step that is counterintuitive to civilians but critical in a combat environment where confusion or TBI can cause a wounded soldier to use their weapon inappropriately.
Available equipment in Phase 2 is still limited to what was carried into the field. There is no resupply. Every intervention must use what is on hand, which is why individual load-out and IFAK contents matter as much as training.
Phase 3 — Tactical Evacuation Care (TACEVAC)
TACEVAC begins when the casualty is being transported to a higher level of care—whether that is a battalion aid station, a forward surgical team, or a Level I trauma center. The threat environment has changed, additional personnel may be available, and more equipment may be accessible.
TACEVAC encompasses two distinct evacuation types:
- CASEVAC (Casualty Evacuation)—movement using armed tactical assets not specifically designated as medical platforms; no Red Cross markings; unregulated movement; combat vehicles, non-medical helicopters
- MEDEVAC (Medical Evacuation)—regulated movement on dedicated medical platforms crewed by medical personnel; ground vehicles or rotary wing; the standard for intra-theater movement to surgical care
In Phase 3, electronic monitoring may be available—pulse oximetry, blood pressure, and continuous cardiac monitoring. Portable fluid warmers and blood products may also be accessible. The treating medic or corpsman transitions from damage control to more comprehensive stabilization, with the goal of presenting the casualty to the receiving surgical team in the best possible condition.
The TCCC card — completed during Phase 2 — becomes the critical handoff document in Phase 3. Surgeons need to know when the tourniquet was applied, what interventions were performed, estimated blood loss, current mental status, and vital trends. A well-documented TCCC card can directly affect what a surgeon decides to do first.
The MARCH Algorithm: TCCC’s Core Assessment Framework
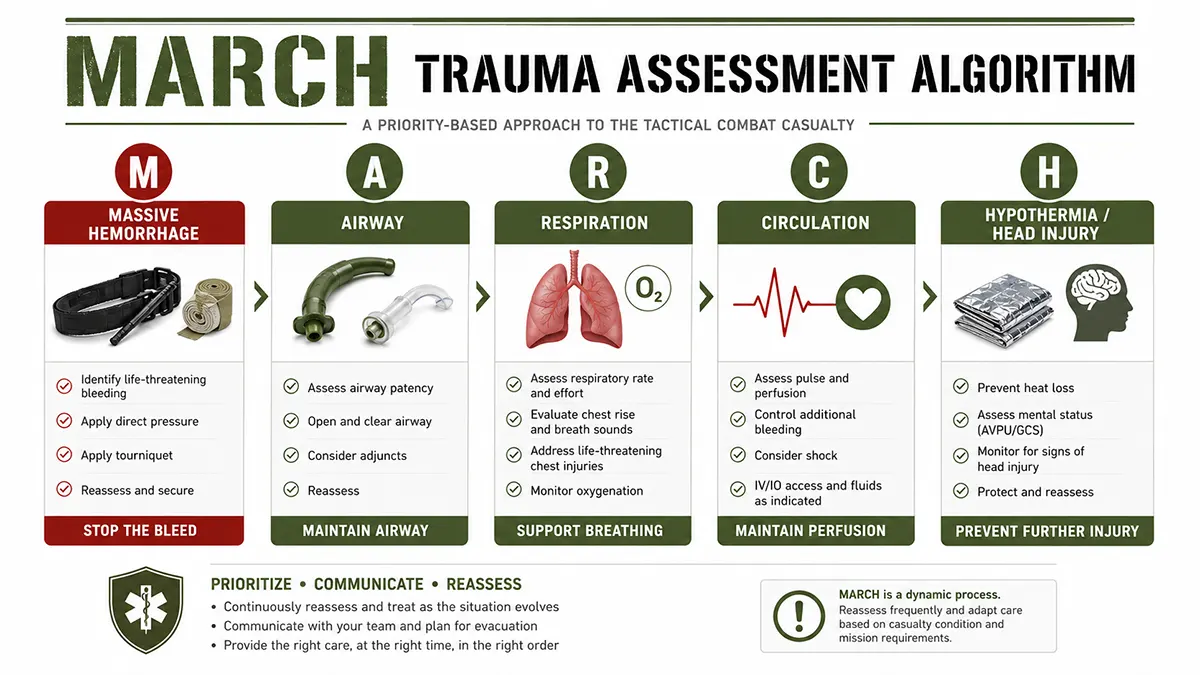
MARCH is the structured assessment sequence used in Phase 2 of TCCC. It prioritizes threats to life in the order they will cause death fastest. Unlike civilian ABC (Airway, Breathing, Circulation), TCCC puts hemorrhage control first—because on a battlefield, compressible bleeding kills faster than airway obstruction in the majority of preventable trauma deaths.
Each letter represents both an assessment and a set of interventions. The sequence is not suggestions—it is the order you work through it, every time, so that under adrenaline and noise and darkness, the decision of what to do next is already made.
| Letter | Stands for | What you are assessing | Key interventions |
|---|---|---|---|
| M | Massive Hemorrhage | Life-threatening external bleeding | CAT tourniquet for limb bleeds; wound packing with hemostatic gauze for junctional wounds; pressure dressings |
| A | Airway | Obstruction or loss of airway patency | Chin-lift / jaw-thrust; NPA for unconscious with intact gag reflex; OPA for fully unconscious; surgical airway if all else fails |
| R | Respiration | Chest injuries reducing oxygenation | Chest seal for penetrating wounds; needle decompression for tension pneumothorax; monitor respiratory rate and quality |
| C | Circulation | Shock from blood loss or cardiac compromise | IV/IO access; blood or fluid resuscitation; assess pulse, skin color, capillary refill; treat hypothermia early |
| H | Hypothermia / Head Injury | Core temperature loss and traumatic brain injury | Warming blanket; monitor GCS, pupil response, and LOC; document neuro status with permanent marker |
Why hemorrhage comes before airway in TCCC
The inversion of MARCH versus ABC is one of the most common questions from people coming from civilian first aid training. The reasoning is based on the epidemiology of preventable combat deaths, not a revision of physiology.
Analysis of combat deaths in Vietnam, the Gulf War, and Operation Enduring Freedom consistently identified compressible hemorrhage—bleeding from limbs and junctional wounds—as the leading cause of preventable battlefield death. Airway obstruction was a smaller fraction of preventable deaths, and most airway deaths occurred in scenarios where rapid surgical care was not available regardless.
The practical implication: stop the bleeding first. A casualty with a controlled tourniquet and a partially compromised airway has time. A casualty with an uncontrolled arterial limb bleed does not.
In civilian trauma settings, the calculus is different. Response times are shorter, surgical care is closer, and the injury patterns differ. Civilian ABC remains appropriate for most non-combat scenarios. TCCC’s MARCH sequence is specifically calibrated to the tactical environment where it was developed.
TCCC vs Civilian First Aid: Key Differences
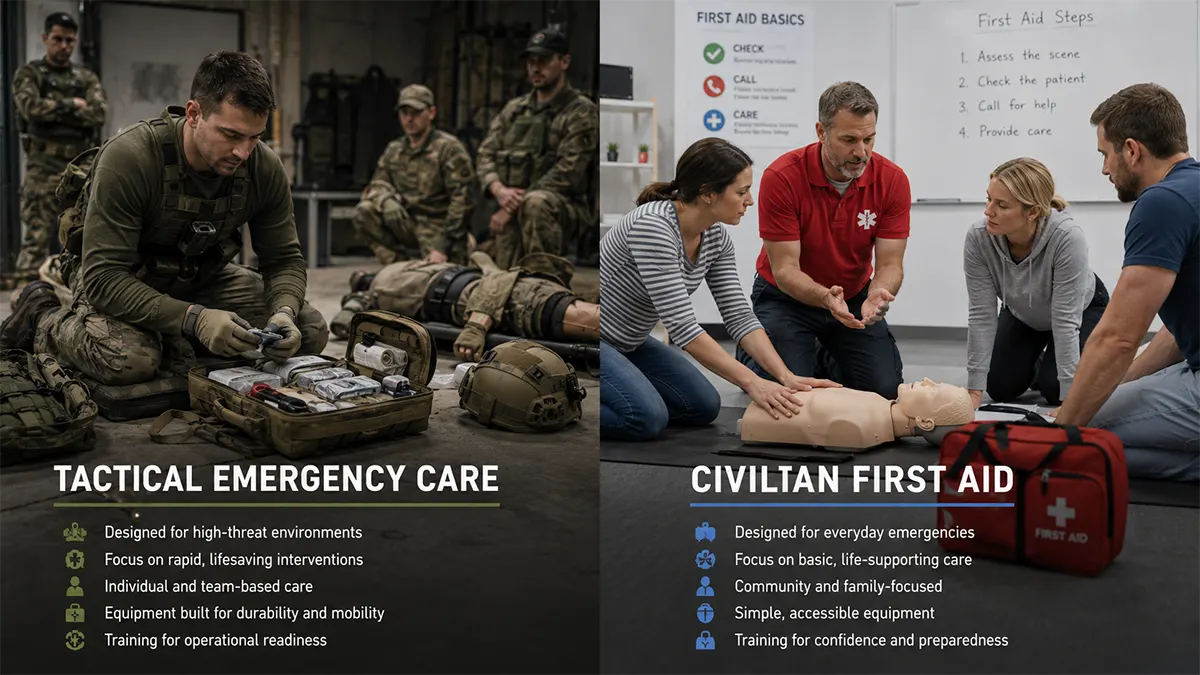
TCCC and civilian first aid share the same fundamental goal—keep the person alive until better care arrives. They differ significantly in the environment they assume, the threat pattern they are designed for, and the protocols they follow as a result.
| Factor | TCCC | Civilian First Aid |
|---|---|---|
| Environment | Active hostile fire; unstable, unpredictable | Generally safe; professional help accessible |
| Medical resources | Only what personnel carry on their person | Ambulances, hospitals, trained responders nearby |
| Primary threat | Compressible hemorrhage, penetrating trauma, blast injury | Cardiac arrest, choking, blunt trauma, medical emergencies |
| Decision authority | Individual soldier/operator makes all treatment calls | First responder stabilizes; EMS assumes care on arrival |
| Protocol structure | MARCH algorithm — strict priority sequence | ABC / DR ABC—more flexible sequencing |
| Treatment priority | Hemorrhage control first, then airway | Airway first, then breathing, then circulation |
| Goal | Keep casualty alive until evacuation to higher care | Stabilize and hand off to professional medical system |
| Who is trained | Military, law enforcement, tactical operators, civilians in Stop the Bleed | General public, CPR/first aid-certified individuals |
The most operationally significant difference for someone training in both systems: in civilian first aid, calling for help is usually the first action. In TCCC Care Under Fire, calling for help may not be possible, may compromise position, or may not result in a faster response than self-evacuation. The rescuer is often the entire medical system available for the first critical minutes.
For law enforcement personnel, TECC (Tactical Emergency Casualty Care) applies TCCC principles to civilian threat environments—active shooter response, mass casualty incidents, and hostile events without military support. The protocols are closely aligned with TCCC but adapted to the legal, organizational, and environmental constraints of civilian law enforcement.
Individual First Aid Kit (IFAK): What TCCC Requires
The IFAK is the individual-level kit that every soldier, operator, and trained civilian carries to execute TCCC interventions. Its contents are organized around the MARCH algorithm—each item addresses a specific threat in the assessment sequence.
The table below reflects a standard TCCC-compliant IFAK build. Specific products will vary by unit, program, and availability. The function each item serves does not.

| Item | MARCH category | Purpose and notes |
|---|---|---|
| CAT Tourniquet (x2 recommended) | M — Massive Hemorrhage | Arterial limb bleed control; one for self-application, one for buddy aid |
| Hemostatic Gauze (kaolin or chitosan) | M — Massive Hemorrhage | Wound packing for junctional or deep bleeding not accessible to tourniquet |
| Pressure Dressing / Israeli Bandage | M — Massive Hemorrhage | Secures packed wounds; applies sustained pressure without hands-on attention |
| Chest Seal (vented, x2) | R — Respiration | Seals penetrating chest wounds; vented design prevents tension pneumothorax development |
| Nasopharyngeal Airway (NPA) + lube | A — Airway | Maintains airway in unconscious casualties with intact gag reflex; NPA is safer in field than OPA for most scenarios |
| Needle Decompression Needle (14g, 3.25″) | R — Respiration | Tension pneumothorax relief; must reach pleural space in larger patients |
| Trauma Shears | All phases | Clothing removal for wound access; should cut through gear without blade exposure risk |
| Permanent Marker | H — Head / Documentation | Time-of-tourniquet application; LOC documentation; TCCC card entries |
| Thermal / Emergency Blanket | H — Hypothermia | Core temperature preservation after blood loss; also signals position |
| TCCC Card / Casualty Card | All phases — Evacuation | Rapid documentation of injuries, interventions, and vitals for handoff to higher care |
| Gloves (nitrile, x2 pairs) | All phases | BSI/infection control; carry two pairs minimum—one pair can tear |
Two notes on IFAK configuration that frequently come up in training:
- Carry two tourniquets. One for self-application, one for buddy aid. Bilateral limb injuries require two simultaneous applications. This is not a redundancy recommendation — it is the standard.
- The kit is designed to be used by someone else on you. Your IFAK position on your body should allow a buddy to access it without moving you significantly. Outside the thigh pouch or chest carrier are standard locations.
Who Should Learn TCCC — and to What Level
TCCC training exists at several levels, and the right level depends on your role and environment. The distinction matters because each level requires different time investment, different skill verification, and different equipment.
TCCC-MP (Medical Personnel)
The full TCCC curriculum, designed for combat medics, corpsmen, pararescuemen, and unit-level medical personnel. Covers the complete three-phase framework, advanced airway management, needle decompression, fluid resuscitation, burn management, and prolonged field care scenarios. Typically 16–40 hours of instruction plus simulation.
TCCC-AC (All Combatants)
The core individual soldier curriculum—the skills every person in a tactical environment needs regardless of medical role. Tourniquet application, wound packing, chest seal application, casualty movement, and MARCH assessment at the layperson level. Typically 4–8 hours. This is the minimum standard for anyone carrying an IFAK into a tactical environment.
Civilian equivalents: Stop the Bleed and TECC
Stop the Bleed is the American College of Surgeons’ adaptation of TCCC hemorrhage control principles for civilian responders—no military context, no tactical framework, just: recognize severe bleeding, apply a tourniquet or pack a wound, and call for help. A two-hour course. This is the appropriate entry point for civilians, teachers, office workers, and anyone who wants to be able to respond to a traumatic bleeding emergency without military training.
TECC (Tactical Emergency Casualty Care) applies the full TCCC three-phase framework to law enforcement, fire/EMS operating in warm zones, and mass casualty responders. It is the recommended training standard for sworn officers and tactical support personnel operating in environments where gunfire or active threats are possible.
Finding a course: The Committee on TCCC (CoTCCC) at deployedmedicine.com maintains a course directory. The National Association of Emergency Medical Technicians (NAEMT) offers PHTLS (Prehospital Trauma Life Support) courses that incorporate TCCC principles. For Stop the Bleed, the American College of Surgeons bleedingcontrol.org lists certified training centers by location.
What TCCC Training Actually Develops

The clinical skills taught in TCCC—tourniquet application, wound packing, chest seal placement, and needle decompression—are learnable in hours. What training actually develops, and what most written guides cannot fully convey, is performance under stress.
Fine motor skills degrade under adrenaline. A tourniquet application that takes 25 seconds in a calm training environment takes 90 seconds the first time a person does it with simulated fire, smoke, darkness, and a screaming casualty. That gap — between trained skill and stress-degraded performance — is what repetition closes.
TCCC training uses scenario-based simulation to create performance conditions close to real: time pressure, noise, incomplete information, multiple casualties, and darkness. The goal is not just that you know the steps. It is that you can execute them when your hands are shaking and every instinct is telling you to run.
Beyond individual skills, TCCC training builds team coordination—who calls for evacuation, who provides covering fire, who treats, and how casualty status is communicated up the chain. These are not instinctive behaviors. They require deliberate practice in team configurations.
Minimum proficiency standard for TCCC-AC: Tourniquet application in under 60 seconds, one-handed, eyes closed. Wound packing and pressure dressing application with correct technique. Correct the MARCH sequence recitation under time pressure. If you cannot meet these standards, you have had instruction but not training.
Recommended Equipment for TCCC Training and Deployment
The equipment recommendations below reflect what we specify for TCCC training programs and deployable IFAKs. Each recommendation includes the specific reason for selection — not just the product name.
Hemorrhage Control
CAT Tourniquet with Metal Windlass Rod (for training use)—We specify the metal windlass version for dedicated training units because polymer windlass rods are rated single-use under occlusion load. A metal rod training unit withstands hundreds of training applications without structural degradation, which significantly reduces per-use training costs. Keep training units clearly marked and physically separated from deployable polymer-windlass units.
Kaolin Hemostatic Gauze — Kaolin-impregnated gauze is the CoTCCC-recommended standard for wound packing. It promotes clotting without the exothermic reaction associated with earlier zeolite-based products. Select a 4-inch wide roll for standard wound packing depth. Confirm the product is OMRI-listed as medical grade before procurement.
Airway Management
Nasopharyngeal Airway (NPA) with Lubricant—The NPA is the standard TCCC airway adjunct because it can be used in conscious and semi-conscious casualties who retain a gag reflex. Size 28 French is the most commonly carried size for adult casualties. Always carry lubricant—dry NPA insertion causes mucosal trauma and patient resistance that complicates the procedure.
Chest Wound Management
Vented Hydrogel Chest Seal (x2) — Carry two: one for entry, one for exit. The vented design allows air to escape from the pleural space while preventing re-entry, reducing the risk of tension pneumothorax development after sealing. Hydrogel adhesive maintains seal in wet or bloody conditions better than foam-backed designs.
For complete kit builds, product specifications, and bulk procurement inquiries, contact our team directly. We work with law enforcement agencies, training programs, and institutional buyers on IFAK configuration specific to their operational environment and training baseline.
Frequently Asked Questions
What does TCCC stand for?
Tactical Combat Casualty Care. It is the evidence-based pre-hospital trauma care framework developed by the U.S. military and maintained by the Committee on Tactical Combat Casualty Care (CoTCCC). The current guidelines were last updated in January 2024.
What are the three phases of TCCC?
Care Under Fire (Phase 1) — treatment while under direct hostile fire, limited to tourniquet application and moving to cover. Tactical Field Care (Phase 2)—systematic assessment and intervention using the MARCH algorithm once the immediate threat is suppressed. Tactical Evacuation Care (Phase 3) — continued care during transport to a higher level of medical treatment.
What is the MARCH algorithm?
MARCH stands for Massive Hemorrhage, Airway, Respiration, Circulation, Hypothermia/Head Injury. It is the structured assessment sequence used in Phase 2 of TCCC, prioritizing threats to life in the order they will cause death fastest. Hemorrhage comes before airway—the inverse of civilian ABC—because compressible bleeding is the leading cause of preventable combat death.
How is TCCC different from civilian first aid?
The core difference is the environment each is designed for. TCCC assumes active threat, limited resources, and a casualty who may not receive professional medical care for an hour or more. Civilian first aid assumes a safe environment, available emergency services, and rapid handoff to professional responders. The intervention priorities differ accordingly—TCCC prioritizes hemorrhage control first; civilian first aid prioritizes airway first.
Can civilians learn TCCC?
Yes. The Stop the Bleed program teaches the core hemorrhage control skills from TCCC — tourniquet application and wound packing — in a two-hour course designed for people with no medical background. TECC (Tactical Emergency Casualty Care) applies the full TCCC framework to civilian and law enforcement contexts. Full TCCC-AC training is available to civilians through NAEMT-certified courses and tactical medicine training programs.
What is in a TCCC-compliant IFAK?
A standard TCCC IFAK includes: tourniquet (x2 recommended), hemostatic gauze, pressure dressing, vented chest seal (x2), nasopharyngeal airway with lubricant, needle decompression needle, trauma shears, permanent marker, thermal blanket, gloves, and a TCCC card. Contents are organized around the MARCH assessment sequence so each item addresses a specific life threat in priority order.
How often should TCCC skills be practiced?
The CoTCCC recommends monthly proficiency practice for personnel carrying IFAKs in operational environments. The minimum standard for TCCC-AC is tourniquet application in under 60 seconds, one-handed, with correct windlass technique. Skills that are not practiced degrade — particularly fine motor skills under stress, which are the first to fail when adrenaline is present.
References
Butler, F.K., Hagmann, J., Butler, E.G. (1996). “Tactical Combat Casualty Care in Special Operations.” Military Medicine, 161(S1), 3-16. The foundational paper establishing TCCC principles.
Committee on Tactical Combat Casualty Care (CoTCCC). TCCC Guidelines for Medical Personnel and All Combatants, January 2024. deployedmedicine.com
Kotwal, R.S. et al. (2011). “Eliminating Preventable Death on the Battlefield.” Archives of Surgery, 146(12), 1350-1358. Documents the reduction in case fatality rate attributable to TCCC implementation.
Kragh, J.F. et al. (2008). “Practical Use of Emergency Tourniquets to Stop Bleeding in Major Limb Trauma.” Journal of Trauma, 64(2 Suppl), S38-S50.
Joint Trauma System, “Tactical Combat Casualty Care Guidelines,” jts.health.mil, 2024
National Association of Emergency Medical Technicians (NAEMT), PHTLS: Prehospital Trauma Life Support, 10th Edition. Incorporates TCCC guidelines for civilian and military pre-hospital providers.
American College of Surgeons — Stop the Bleed Program. bleedingcontrol.org
Disclaimer: This article is for educational purposes only and does not constitute medical advice. TCCC skills should be learned and practiced under qualified instruction. In a medical emergency, call emergency services immediately.

